Primary Alveolar Echinococcosis of the Kidney
Rare case of primary renal AE in a 67-year-old asymptomatic Moroccan man
15/12/2025
Esselmani H – Kidney Alveolar Echinococcosis
Hicham Esselmani[1], Rachid Hnini[1], Eliane Silva[2], Mustapha Najimi[3],[4] and Mohamed Merzouki[1]
[1]. Sultan Moulay Slimane University, Faculty of Science and Technology, Biological Engineering Laboratory, Beni Mellal, Morocco.
[2]. University of Porto, School of Medicine and Biomedical Sciences, Porto, Portugal.
[3]. University Catholic of Louvain, Institute of Experimental and Clinical Research, Laboratory of Pediatric Hepatology and Cell Therapy, Brussels, Belgium.
[4]. Private University of Marrakech, Morocco.
Corresponding author: Dr. Hicham Esselmani. E-mail: esselmani1@yahoo.fr
Financial Support: None
Conflict of Interest: The authors declare no conflicts of interest.
Editor: Dalmo Correia Filho
Orcid
Hicham Esselmani: 0000-0001-7074-3369
Rachid Hnini: 0000-0002-8575-8501
Eliane Silva: 0000-0002-9771-8769
Mustapha Najimi: 0000-0002-7329-9635
Mohamed Merzouki: 0000-0002-9837-4312
Alveolar echinococcosis (AE), which is caused by the larval stage of Echinococcus multilocularis, is a rare and aggressive parasitic disease1. Over 95% of cases involve the liver, with primary extrahepatic AE being exceptionally uncommon2. Here, we present a rare case of primary renal AE in a 67-year-old asymptomatic Moroccan man.
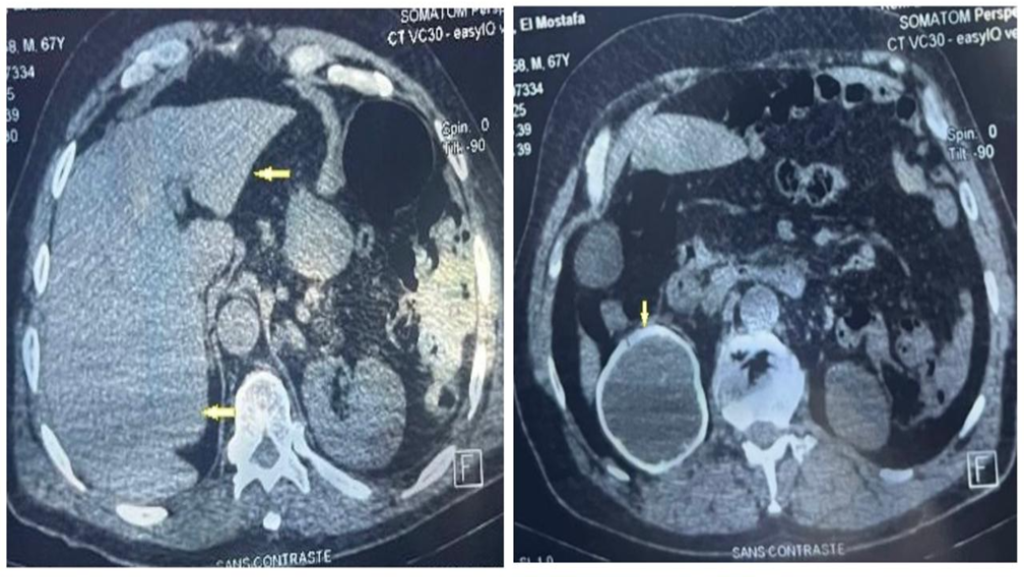
The lesion was incidentally detected on thoraco-abdomino-pelvic computed tomography (CT). Abdominal CT revealed a calcified cystic mass in the right kidney, associated with renal atrophy (Figure 1). The liver and other abdominal organs showed no signs of lesions (Figure 2). Serology using an indirect hemagglutination test for E. granulosus yielded a negative result. However, an Anti-Echinococcus EUROLINE-Western Blot IgG assay tested positive for antibodies against the E. multilocularis-specific antigen Em95 (Figure 3), confirming the diagnosis of AE.
To our knowledge, this represents the first case of primary renal AE reported in Morocco and the second described worldwide3. Isolated renal AE is a clinical mimic that can easily be misdiagnosed as a renal tumor based solely on imaging4. Maintaining a high index of suspicion is essential in non-endemic regions and cases with atypical presentations. Specific immunoblotting is a valuable noninvasive tool for distinguishing AE from other cystic renal lesions and for guiding appropriate management, which typically involves a combination of surgery and long-term albendazole therapy4.
Authors Contributions
HE: Acquisition, analysis, and interpretation of the data, Writing of the original draft, review, and editing. RH, ES, MM, and MN: Revision and interpretation of data, review, and editing. HE, MM, and MN: revision and interpretation of data, review, and editing. MM, MN: supervised the work, contributed to manuscript writing, analysis and interpretation of data, preparation of figures, review and editing, and final approval of the manuscript.
Acknowledgments
The authors sincerely thank all those who contributed to the success of this study.
References
- Kodama Y, Fujita N, Shimizu T, Endo H, Nambu T, Sato N, et al. Alveolar echinococcosis: MR findings in the liver. Radiology. 2003;228:172–7.
- Piarroux M, Piarroux R, Giorgi R, Knapp J, Bardonnet K, Sudre B,et al. Clinical features and evolution of alveolar echinococcosis in France from 1982 to 2007: results of a survey in 387 patients. J Hepatol 2011;55:1025–33.
- Türker Köksal I, Tefekli A, Kiliçaslan I, Erdemir F, Kadioğlu T, Esen T. Hydatid disease of the kidney caused by Echinococcus multilocularis. Urol Int 2001;67:310–312.
- Meinel TR, Gottstein B, Geib V, Keel MJ, Biral R, Mohaupt M, et al. Vertebral alveolar echinococcosis-a case report, systematic analysis, and review of the literature. Lancet Infect Dis. 2018 Mar;18(3):e87-e98.
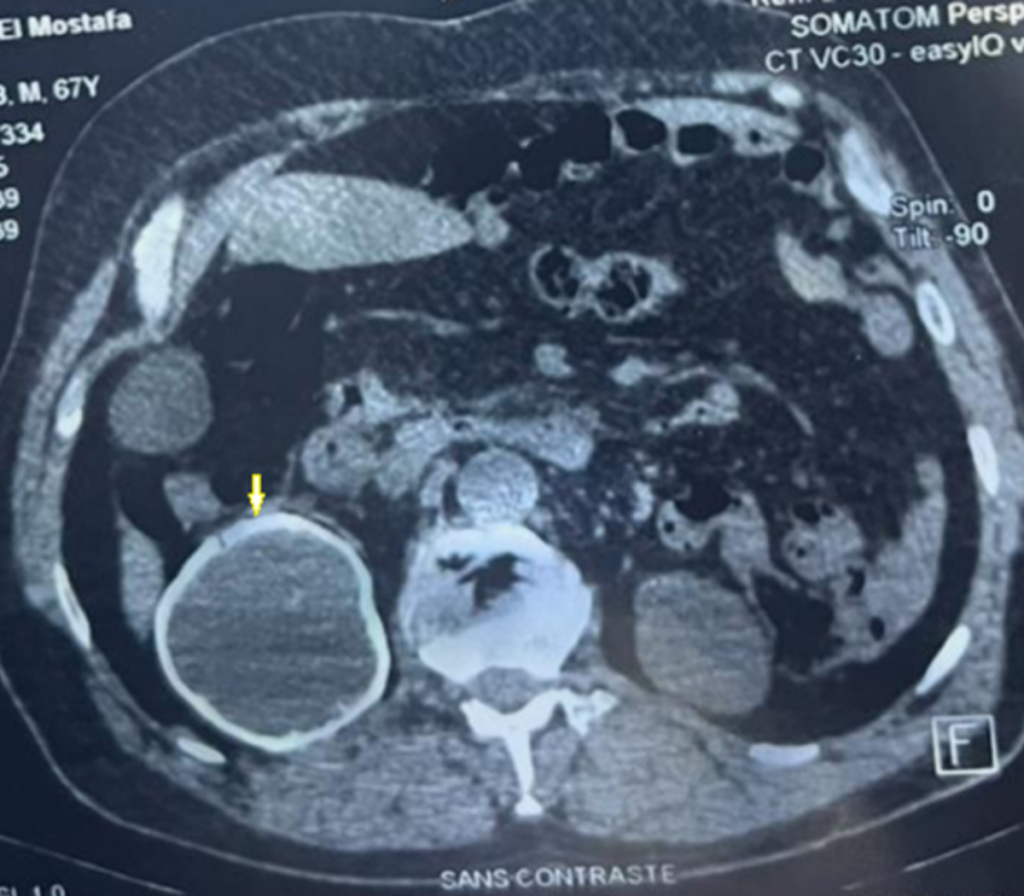
FIGURE 1: Abdominal tomography showing a calcified cyst in the right kidney with atrophy
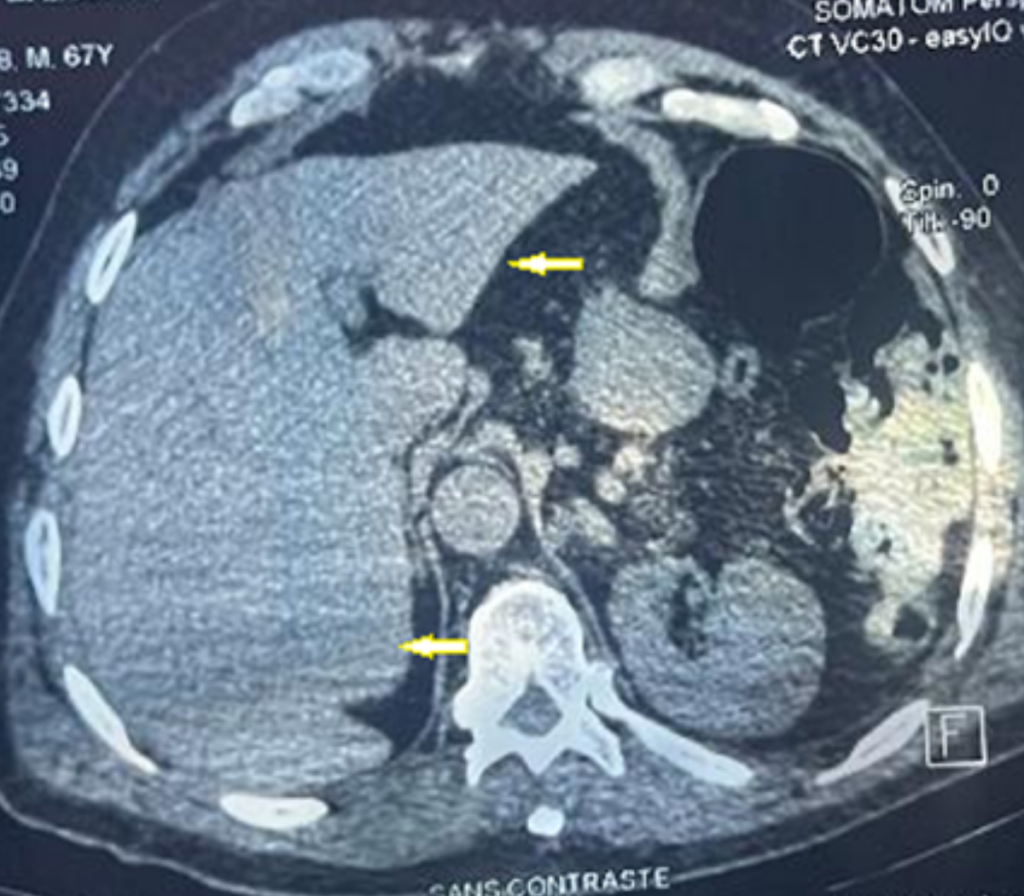
FIGURE 2: Abdominal tomography showing the liver without cystic or solid lesions