Methotrexate-Induced Pneumonitis in a Patient with Chronic Chikungunya Arthritis
09/07/2025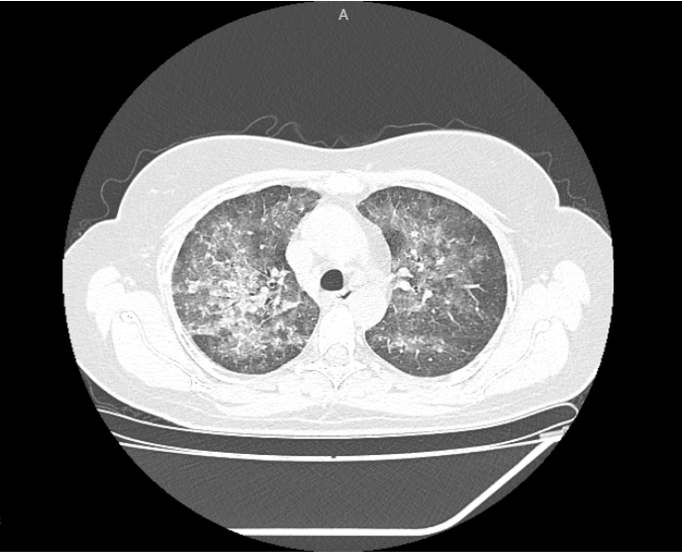
Oliveira JL et al. – MTX-Induced Pneumonitis in Chikungunya Arthritis
Jobson Lopes de Oliveira[1],[2], Igor Albuquerque Nogueira[3], Afonso Rocha Eisele[1] and Luis Arthur Brasil Gadelha Farias[1],[4],[5]
[1]. Centro Universitário Christus, Faculdade de Medicina, Fortaleza, CE, Brasil.
[2]. Universidade Federal do Ceará, Faculdade de Medicina, Departamento de Medicina Clínica, Fortaleza, CE, Brasil.
[3]. Universidade de São Paulo, Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto, Ribeirão Preto, SP, Brasil.
[4]. Universidade de São Paulo, Departamento de Doenças Infecciosas do Hospital das Clínicas, Laboratório de Investigação Médica – LIM 49, São Paulo, SP, Brasil.
[5]. Hospital São José de Doenças Infecciosas, Fortaleza, CE, Brasil
Corresponding author: Jobson Lopes de Oliveira. e-mail: jobsonlopesdeoliveira@gmail.com
Orcid
Jobson Lopes de Oliveira: https://orcid.org/0000-0001-8912-1121
Igor Albuquerque Nogueira: https://orcid.org/0000-0002-3810-672X
Afonso Rocha Eisele: https://orcid.org/0000-0001-8396-4208
Luis Arthur Brasil Gadelha Farias: https://orcid.org/0000-0002-8978-9903
Authors’ contribution: JLO: Conception and design of the study, Acquisition of data, Analysis and interpretation of data, Drafting the article, Final approval of the version to be submitted; IAN: Analysis and interpretation of data, Drafting the article; Final approval of the version to be submitted; ARE: Analysis and interpretation of data, Drafting the article; Final approval of the version to be submitted; LABGF: Analysis and interpretation of data, Drafting the article, Final approval of the version to be submitted.
Financial Support: None
Conflict of Interest: The authors declare no conflicts of interest.
Received 14 April 2025 – Accepted 13 May 2025
Methotrexate (MTX) is a cornerstone in the treatment of inflammatory arthritis owing to its immunomodulatory effects. Its use has expanded to the management of post-viral inflammatory conditions, including chronic arthritis caused by Chikungunya virus (CHIKV) infection, which may mimic rheumatoid arthritis (RA)1. Although effective, MTX poses a risk of adverse effects, including rare but potentially life-threatening complications such as pneumonitis2,3.
We present the case of a 50-year-old Brazilian woman who developed MTX-induced pneumonitis during treatment for post-CHIKV arthritis. Initial presentation included acute-onset fever, rash, and polyarthritis. Serological testing confirmed a recent CHIKV infection (IgM-positive), while investigations for other causes of inflammatory arthritis, including RA and systemic lupus erythematosus, were negative. Symptoms improved with corticosteroids, and MTX (15 mg/week) was initiated as a steroid-sparing agent.
Three weeks later, the patient developed progressive dyspnea, dry cough, and intermittent fever. Infectious etiologies, such as SARS-CoV-2 and HIV, were excluded, and high-resolution computed tomography (CT) revealed diffuse bilateral ground-glass opacities and interlobular septal thickening. These findings were predominantly observed in the upper lobes and peribronchovascular regions, consistent with hypersensitivity pneumonitis (Figure 1). MTX was discontinued. Methylprednisolone pulses was applied, resulting in rapid clinical improvement without symptom recurrence, thus supporting the diagnosis of MTX-induced pneumonitis.
MTX-induced pneumonitis typically manifests as an acute or subacute hypersensitivity reaction, which often occurs within the first year of therapy3. Radiological findings may resemble those of nonspecific interstitial pneumonia, with histopathology revealing lymphocytic infiltrates and non-caseating granulomas.
Given the efficacy of MTX in treating post-CHIKV arthritis, clinicians should be vigilant of pulmonary toxicity, particularly during the early stages of treatment. Risk factors include old age, pre-existing lung disease, diabetes mellitus, and hypoalbuminemia2,3. Early recognition and prompt withdrawal of MTX are crucial for recovery and the prevention of disease progression.
References
References
- Amaral JK, Sutaria R, Schoen RT. Treatment of Chronic Chikungunya Arthritis With Methotrexate: A Systematic Review. Arthritis Care Res (Hoboken). 2018;70(10):1501–8. Available from: https://doi.org/10.1002/acr.23519
- Cottin V, Bendstrup E, Bonniaud P, Nasser M, Spagnolo P, Valenzuela C, et al. The case of methotrexate and the lung: Dr Jekyll and Mr Hyde. Eur Respir J. 2021;57(2):2100079. Available from: https://doi.org/10.1183/13993003.00079-2021
- Fragoulis GE, Nikiphorou E, Larsen J, Korsten P, Conway R. Methotrexate-Associated Pneumonitis and Rheumatoid Arthritis-Interstitial Lung Disease: Current Concepts for the Diagnosis and Treatment. Front Med (Lausanne). 2019;6:238. Available from: https://doi.org/10.3389/fmed.2019.00238
FIGURE 1. High-resolution computed tomography scan of the chest showing diffuse bilateral ground-glass opacities with interlobular septal thickening that predominantly affected the upper lobes and peribronchovascular regions. These radiological features are characteristic but not pathognomonic of MTX-induced pneumonitis.