Paracoccidioidomycosis: An uncommon cause of discitis in lupus
Appenzeller S et al. - Paracoccidioidomycosis: An uncommon cause of discitis
12/08/2024Simone Appenzeller[1], Lilian Lavras Costallat[1], Marcelo de Carvalho Ramos[2], Samuel de Oliveira Andrade[1] and Fabiano Reis[3]
[1]. Universidade Estadual de Campinas, Departamento de Ortopedia, Reumatologia e Traumatologia, Campinas, SP, Brasil.
[2] Universidade Estadual de Campinas, Departamento de Clínica Médica, Campinas, SP, Brasil.
[3]. Universidade Estadual de Campinas, Departamento de Anestesiologia, Oncologia e Radiologia, Campinas, SP, Brasil.
Corresponding author: Dr. Fabiano Reis. e-mail: fabianoreis2@gmail.com
Authors’ contribution
SA: acquisition of data and writing the initial drafts of the manuscript; LLC: acquisition of data and writing the initial drafts of the manuscript; MCR: acquisition of data and critical revision; SOA: acquisition of data and critical revision; FR: concept, acquisition of data and critical revision of the manuscript for intellectual content.
Conflict of Interest
The authors have no conflict of interest with this work.
Financial Support
There is no funding sources.
Orcid
Simone Appenzeller: https://orcid.org/0000-0001-5075-4474
Lilian Lavras Costallat: https://orcid.org/0000-0002-3077-9479
Marcelo de Carvalho Ramos: https://orcid.org/0000-0002-1532-1849
Samuel de Oliveira Andrade: https://orcid.org/0000-0001-7222-9953
Fabiano Reis: https://orcid.org/0000-0003-2256-4379
Received 2 June 2024 – Accepted
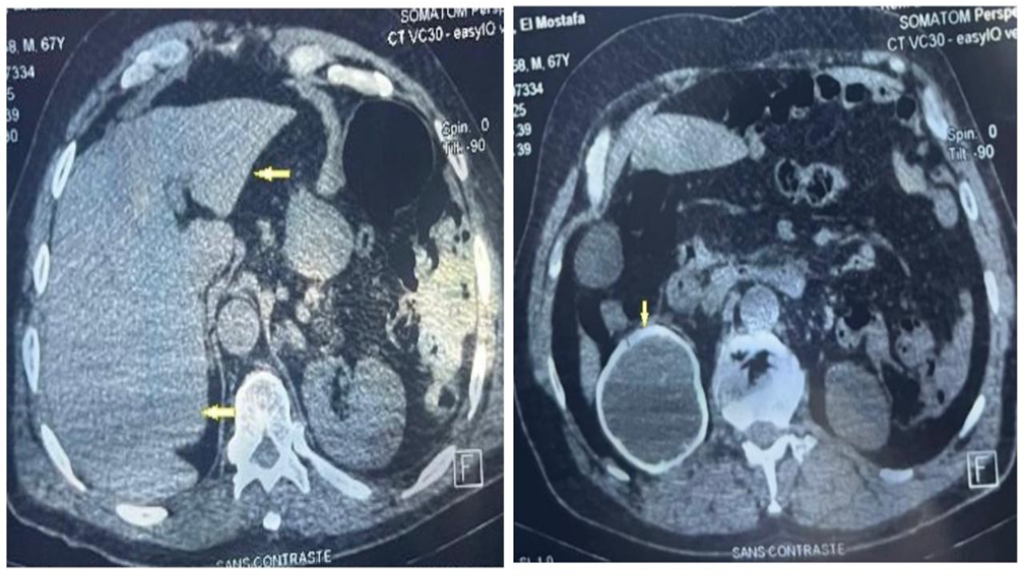
A 41-year-old woman with systemic lupus erythematosus (SLE) presented to the outpatient department with progressive 3-month interscapular pain that was refractory to analgesics. The patient’s medications included azathioprine 50 mg, hydroxychloroquine 400 mg, and prednisone 5 mg daily. She reported a weight loss of 7 kg in the previous 2 months but denied experiencing fever or any history of trauma. She lived in a rural area and worked in the agricultural sector. Thoracic spinal radiographs obtained during the initial assessment revealed T7 vertebral collapse and diffuse nodular pulmonary opacities. The patient was hospitalized; chest computed tomography (CT) revealed the presence of diffuse micronodular disease (Figure 1) and vertebral collapse associated with signs of spondylodiscitis at T6–T7 and T7–T8, which were confirmed by magnetic resonance imaging (Figures 2 and 3). A T8 paravertebral computed tomography-guided biopsy confirmed the presence of Paracoccidioides spp. The patient was treated with itraconazole 100 mg daily for 3 months, resulting in the complete resolution of infection and a good outcome.
Active disease and immunosuppressive therapy are risk factors for infection in patients with SLE1. Invasive fungal infections usually occur in immunocompromised hosts, with the most common pathogens in SLE patients being Candida albicans, Cryptococcus neoformans, and Aspergillus spp.2,3. Osteoarticular involvement in paracoccidioidomycosis is unusual, mainly affecting the bones of the chest wall (ribs, sternum, scapula, and acromion). Discitis-osteomyelitis, particularly when caused by fungi, is a rare infection4. To our knowledge, only two patients with vertebral body paracoccidioidomycosis have been reported in the literature5.
Acknowledgments
We offer our deepest thanks to the institutions that provided technical support for the development and implementation of this study.
References
- Danza A, Ruiz-Irastorza G. Infection risk in systemic lupus erythematosus patients: susceptibility factors and preventive strategies. Lupus. 2013;22(12):1286-94.
- Ruiz-Irastorza G, Olivares N, Ruiz-Arruza I, Martinez-Berriotxoa A, Egurbide MV, Aguirre C. Predictors of major infections in systemic lupus erythematosus. Arthritis Res Ther. 2009;11(4):R109.
- Lao M, Wang X, Ding M, Yang Z, Chen H, Liang L, et al. Invasive fungal disease in patients with systemic lupus erythematosus from southern China: a retrospective study. Lupus. 2019;28(1):77-85.
- Miyoshi IC, de Toledo AHN, Pereira FV, Villarinho LL, Dalaqua M, de Ávila Duarte J, et al. Infectious myelitis. Semin Ultrasound CT MR. 2023;44(5):424-35.
- Alvarenga JA, Martins DE, Kanas M, Elizeche HG, Dell’Aquila AM, Fernandes EA, et al. Paracoccidioidomycosis in the spine: case report and review of the literature. São Paulo Med J. 2016;134(3):263-67.
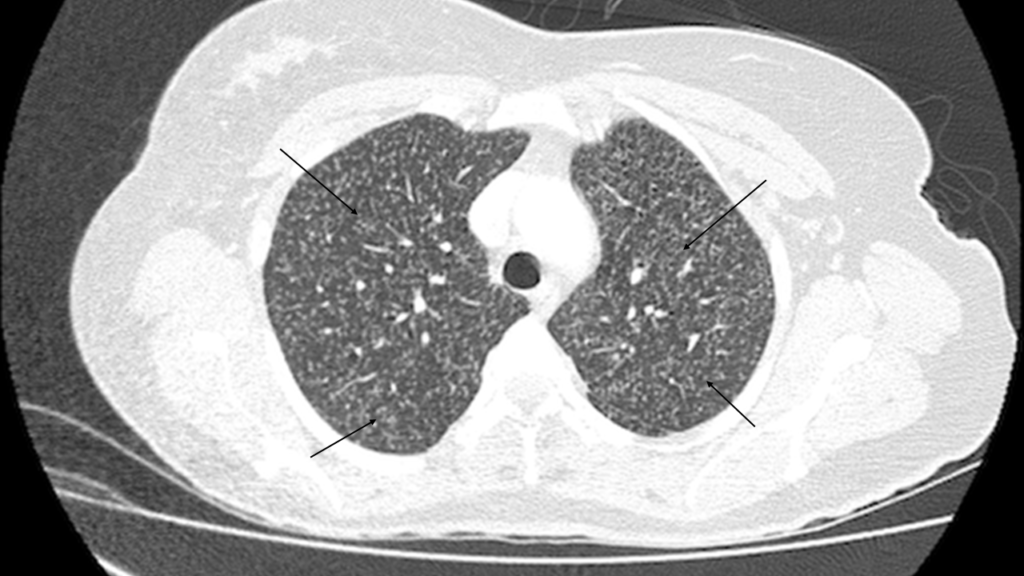
FIGURE 1: Chest computed tomography, with the axial pulmonary window showing multiple randomly distributed pulmonary micronodules (arrows) in both lungs

FIGURE 2: Magnetic resonance imaging. Sagittal T2 short tau inversion recovery showing the hyperintensity of the T6–T7 intervertebral disk and the absence of the internuclear cleft. Hyperintensity of the adjacent vertebral bodies was also observed. The lesion posteriorly compressed the dural sac and the spinal cord (arrow).

FIGURE 3: Magnetic resonance imaging. Sagittal contrast-enhanced T1-weighted fat-suppressed MR weighted image of the thoracic spine showing paravertebral collections with peripheral enhancement, enhancement of the T6 and T8 vertebral bodies (arrow), a necrotic collapsed T7 vertebral body, and a posterior epidural mass with peripheral enhancement at the T4–T7 levels, suggesting epidural abscess. An anterior epidural collection at the T7 level combined with angular kyphosis resulted in spinal cord compression (arrow).