Renal abscess in a patient with a long-term double-J stent due to Candida albicans
Memiş KB et al. - Unusual renal abscesses
12/08/2024Kemal Buğra Memiş[1], Muktedir Emir Şahin[1], Volkan Kızılgöz[1], Ali Osman Gülmez[1] and Sonay Aydın[1]
[1]. Erzincan University, School of Medicine, Department of Radiology, Erzincan, Turkey.
Corresponding author :Muktedir Emir Şahin, MD. e-mail: m.emirsahinn@gmail.com
Authors’ contribution
KBM: Conception and design of the study, Acquisition of data, Supervision, Materials, Data collection, Writing, Final approval of the version to be submitted, Critical review contribution type; MES: Conception and design of the study, Materials, Final approval of the version to be submitted, Literature review, Writing; SA: Conception and design of the study, Analysis and interpretation of data, Drafting the article, Final approval of the version to be submitted, Writing, Critical review contribution type.
Conflict of Interest
The authors assert that they have no conflict of interest.
Financial Support
This study did not receive any financial support from external sources.
Orcid
Kemal Bugra Memis: https://orcid.org/0009-0007-6746-3906
Muktedir Emir Şahin: https://orcid.org/0009-0003-4679-9778
Sonay Aydın: https://orcid.org/0000-0002-3812-6333
Volkan Kızılgöz : https://orcid.org/0000-0003-3450-711X
Ali Osman Gülmez: https://orcid.org/0000-0001-7050-1765
Received 11 June 2024 – Accepted 24 June 2024
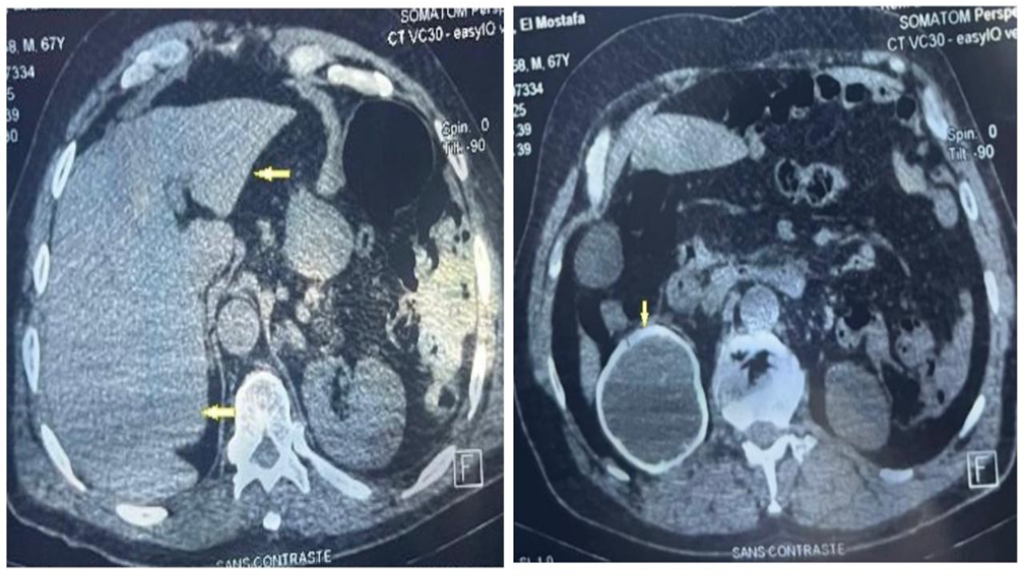
A 39-year-old male patient underwent right hemicolectomy and double-J stent placement for penetrating abdominal trauma that resulted in ureter and bowel injuries. Contrast-enhanced abdominal computed tomography revealed grade 3 hydronephrosis of the right kidney and a double-J catheter. Furthermore, a substantial amount of intrarenal fluid was detected in the lower pole of the right kidney, leading to decreased perfusion of the surrounding renal tissue and inflammation of the pararenal adipose tissue (Figure 1). Sonoelastography of the right kidney showed that the lesion predominantly consisted of soft stromal structures (Figure 2). Treatment was initiated specifically upon Candida albicans detection in the urine culture. Repeated imaging revealed a reduction in the lesion size, and complete recovery was achieved without percutaneous drainage.
Candida albicans is a component of the normal microflora in the gastrointestinal tract of humans1. The disruption of the skin and digestive barriers can lead to invasive diseases2,3. In healthy adults, Candida is detected in less than 1% of clean urine samples; however, in hospitals, it is typically detected in 5%–10% of positive urine cultures, particularly in patients with bladder catheters4,5. Candida-related renal abscesses are characterized by localized pus in the renal parenchyma and often present with fever, flank pain, and septicemia2,3,6. Prompt imaging and antifungal treatments, such as fluconazole, are essential to prevent complications6. Candida infections should be considered in complex renal lesions in patients with a history of bladder catheterization or gastrointestinal perforation.
Acknowledgements
The authors thank the research staff at the Radiology Department of Erzincan University for their valuable assistance.
References
- Talapko J, Juzbašić M, Matijević T, Pustijanac E, Bekić S, Kotris I, et al. Candida albicans-The Virulence Factors and Clinical Manifestations of Infection. J Fungi (Basel). 2021;7(2):79.
- Chang CY, Jayabalan M, Gan YL, Radhakrishnan AP, Ong ELC. Enterococcus hiraebacteremia associated with perinephric collection and renal abscesses in a diabetic woman. Oxf Med Case Reports. 2022;2022(9):omac101.
- Pappas PG, Lionakis MS, Arendrup MC, Ostrosky-Zeichner L, Kullberg BJ. Invasive candidiasis. Nat Rev Dis Primers. 2018;4:18026.
- Alfouzan WA, Dhar R. Candiduria: Evidence-based approach to management, are we there yet? J Mycol Med. 2017;27(3):293-302.
- Kauffman CA, Vasquez JA, Sobel JD, Gallis HA, McKinsey DS, Karchmer AW, et al. Prospective multicenter surveillance study of funguria in hospitalized patients. The National Institute for Allergy and Infectious Diseases Mycoses Study Group. Clin Infect Dis. 2000;30(1):14-8.
- Fisher JF, Sobel JD, Kauffman CA, Newman CA. Candida urinary tract infections–treatment. Clin Infect Dis. 2011;52(Suppl 6):S457-66.
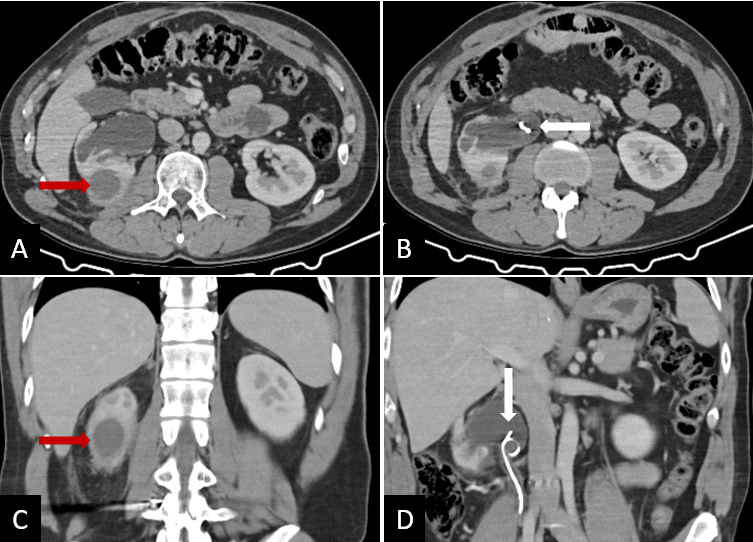
FIGURE 1: Axial (A–B) and coronal (C–D) plane enhanced abdomen computed tomography shows a well-defined collection resembling an abscess in the right kidney. The collection has a diameter of 3 cm at its lower pole (red arrows). Additionally, grade 3 hydronephrosis and double-J stent are observed in the right kidney (white arrows).

FIGURE 2: Longitudinal gray scale (A), color Doppler (B) ultrasound, and shear-wave elastography (C) images of the lesion in the right kidney. Doppler ultrasonography shows a hypoperfused lesion in the renal parenchyma of the right kidney. The sonoelastography images showed the soft stromal structures (red arrows).